Transcript
Announcer:
Welcome to CME on ReachMD. This episode is part of the Global Heart Failure Academy and is brought to you by Medtelligence.
Prior to beginning the activity, please be sure to review the faculty and commercial support disclosure statements as well as the learning objectives.
Dr. Giuseppe Rosano:
Iron deficiency in heart failure is a common comorbidity. The evidence for IV iron treatment in patients with heart failure continue to grow and it informs our guideline recommendations. So what impacts the clinical evidence? And what is the value of this evidence for our patients?
This is CME on ReachMD, and I’m Dr. Giuseppe Rosano.
Dr. Ovidiu Chioncel:
I’m Dr. Ovidiu Chioncel.
Dr. Antoni Bayés-Genís:
And I’m Dr. Toni Bayés-Genís.
Dr. Giuseppe Rosano:
So I would like to first discuss the guideline recommendations I just mentioned. I'll tell you about the recent updates to the ESC guidelines and how they relate to treating patients with heart failure and iron deficiency.
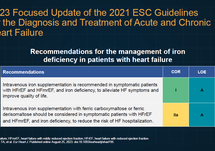
So we know that the updates to the ESC guidelines, they specifically, for what they pertain, IV irons in patients with heart failure, they gave a class IA recommendation to alleviate symptoms and improve quality of life. And then there's a second recommendation, is a class IIa, A for ferric carboxymaltose or ferric derisomaltose to reduce the risk of rehospitalizations.
So the update of the guidelines is also based on the new evidence that came with IRONMAN. IRONMAN was a large study with ferric derisomaltose. And in patients with heart failure, that slightly different classifications for or definitions for iron deficiency. As previous studies, has been affected by COVID, but the COVID sensitivity analysis, also in this case, demonstrated a significant effect on the primary endpoint. So putting together the data from IRONMAN with that data of evidence has been gained over the years with ferric carboxymaltose led to meta-analysis that confirmed the clear effect of IV iron in reducing the composite endpoint of heart failure hospitalizations and cardiovascular events. This was mainly driven by the effect on heart failure hospitalizations, but nevertheless, this is very important because heart failure hospitalizations are clearly a very important endpoint in patients with heart failure.
All the evidence that came from all the trials also led to a class IA recommendation because of this very significant effect of IV iron. Again, most of the data driven by the studies with ferric carboxymaltose on quality of life and exercise capacity. And there was a class IIa, that was for the reduction of hospitalizations where the data of the previous data with ferric carboxymaltose, strong data with ferric carboxymaltose, were also put together with the data with ferric derisomaltose. And therefore, we have 2 new recommendations that are very important for clinical practice because they will guide treatment not just for the prognosis for patients with heart failure, but also for the quality of life and exercise capacity.
So we will be discussing this evidence. And first of all, I would like to have your comments on what you think is the impact of this change in the guideline recommendations.
Dr. Ovidiu Chioncel:
First of all, I would like to say that it's a huge update in terms of clinical practice for how to use in clinical practice IV ferric carboxymaltose for patients with heart failure with reduced ejection fraction, mildly reduced ejection fraction. Beyond of how much ferric carboxymaltose is decreasing heart failure hospitalization, time to first hospitalization, it's very, very important, in my opinion, improving quality of life, because patients with heart failure have a very poor quality of life; they have low functional capacity. And this is a moment when we set up new threshold for patients with reduced and mildly reduced ejection fraction to improve these clinically relevant endpoints.
Dr. Antoni Bayés-Genís:
Yeah, Giuseppe, I think this is an important topic. If we go to the probability of having iron deficiency, we see that in chronic heart failure, it's affecting close to 50% of patients. And in the setting of acute heart failure, it’s close to 90% of patients. So we need to give clear recommendations to the guidelines and the guidelines with the evidence, up to the time of the guidelines, and then we can discuss the new evidence, was very supportive of IV iron in iron deficiency patients in spite of anemia. So it's changing times. But certainly, it's very prevalent, and we need to take that into account.
Dr. Giuseppe Rosano:
So, Ovidiu, we've seen considerable data over the years for the use of IV iron, mostly with ferric carboxymaltose, in our iron-deficient patients with heart failure. Now let's talk about what we've learned in the HEART-FID and what were the results and what can we learn from the outcome of the trial. But importantly, what do you think is the real value of the P value set by the regulators?
Dr. Ovidiu Chioncel:
Thank you so much, Giuseppe. I think that HEART-FID, it's a very important clinical trial. First of all, it's a largest randomized clinical trial to assess mortality and readmission in patients with heart failure and reduced ejection fraction, as Tony said, irrespective of anemia. Actually, HEART-FID, randomized 3,000 patients, 1,500 receiving IV ferric carboxymaltose, the rest being treated with placebo. Very interesting in terms of study design was recurrent IV ferric carboxymaltose administration protocol was based not on Ganzoni formula, but on level of hemoglobin and bodyweight. And this is interesting and easily applicable in clinical practice for all level of clinical settings. Endpoint was a hierarchical composite including 12 months death, 12 months heart failure hospitalization, and change from baseline of 6-minutes walking test. The results were positive when compared to absolute risk reduction because the IV ferric carboxymaltose decreased the number of deaths. IV carboxymaltose decreased the number of heart failure hospitalizations and prolonged the time to first heart failure hospitalization, and even more, at 6 months, increased about 4 meter distance in 6-minutes walking test.
We should see this trial in the large context of totality of evidence, what we have till now, what this clinical trials brings to us. And I think that we have a lot of data. I will not be impressing this stage of P value, because a trend for all endpoints, primary endpoints, and also for secondary endpoints when things are same direction. Also for cardiovascular deaths, also for composite of cardiovascular deaths and heart failure hospitalization, all will land in the same direction. So I think that it's important brick to the wall for evidence of treating iron deficiency with IV ferric carboxymaltose in patients with heart failure and reduced ejection fraction.
Dr. Giuseppe Rosano:
So for those just tuning in, you're listening to CME on ReachMD. I'm Dr. Giuseppe Rosano. And here with me today are Dr. Ovidiu Chioncel and Dr. Antoni Bayés-Genís. We're discussing recent ESC guidelines updates and the totality of evidence for the use of IV iron in our patients with heart failure.
No, I agree with you. And also what is important is that the statistical significance is always set based on statistical values, and then the regulators may decide to set other standards for their approval. But that is not the scientific value of the P. So from a statistical point of view, it's that pure statistically that is a positive trial. Maybe it didn't meet the regulators’ requirements. But that is a completely different issue. So we have to, here, to dissect and divide, in my opinion, what is science from what is regulators’ requirement? And from a scientific point of view, I think that the trial was very significant.
Dr. Antoni Bayés-Genís:
Yeah, I think what you both said is right; nevertheless, we need to go to the conclusions of the trial, which were neutral, and we need to put these uncertainties in the whole context. And this will probably require additional trials, there is the FAIR-HF2 ongoing, and I think that the whole incorporation of the 4 trials prior to HEART-FID plus FAIR-HF2 will give us a very nice overview. But to me, despite what you're saying, the result was a little bit disappointing, and I was expecting a very clear, neat, positive trial. But anyway, as you say, clinically, the results are significant.
Dr. Giuseppe Rosano:
So, Tony, now I would like to hear you talk, because you discussed about the totality of the evidence and we have to look at the totality of the evidence. So we have the recent meta-analysis with the use of IV iron in patients with heart failure and iron deficiency. Now how do the data impact the current body of evidence, and what is the value of using IV iron to treat our iron-deficient patients with heart failure?
Dr. Antoni Bayés-Genís:
Yeah, yeah, that's a good study that has been reported recently and published that evaluated 4 trials: HEART-FID, AFFIRM, CONFIRM with ferric carboxymaltose, and IRONMAN with ferric derisomaltose. The first 3 trials, investigators could analyze individual patient data. For the IRONMAN it was study-level data. What they did is to go to composite endpoint of heart failure hospitalization plus death and to study these in the meta-analysis. Very interestingly, the results taken in the forest plot are very significant in benefit of IV iron treatment. And these are the very good news. When they use a Bayesian approach, they do see some degree of uncertainty for future trials, and the investigators suggest that this meta-analysis needs to be completed with FAIR-HF2, but the evidence is very positive for IV iron. And there is no significant differences according to subgroups. No significance between sex, between ischemic or non-ischemic etiology, renal function, New York Heart Association class, transferrin saturation. So overall, I would say that the evidence that we have in this meta-analysis is supporting the guideline Recommendation 1A.
Dr. Giuseppe Rosano:
Ovidiu, we have heard Tony's thoughts on the meta-analysis. Do you have any other comment?
Dr. Ovidiu Chioncel:
Yes, Giuseppe, I would like to say about what clinicians should keep in mind about the results of this meta-analysis. And I would like to say that the final message should be the net result is positive. We should improve quality of life, as you said, functional capacity treating iron deficiency with ferric carboxymaltose or derisomaltose in patients with reduced and mildly reduced ejection fraction without affecting cardiovascular mortality and heart failure hospitalization, but even more with a trend to be positively influenced. This is a strong message from my side for all clinicians to use IV ferric carboxymaltose and IV ferric derisomaltose in patients with reduced and mildly reduced ejection fraction. On the other hand, improving quality of life, it's a clinically relevant endpoint. And we all know very well that patients with severe heart failure sometimes trade off quality of life with years of survival.
Dr. Giuseppe Rosano:
Tony, any comment from your side?
Dr. Antoni Bayés-Genís:
Yeah, yeah, Giuseppe. I think it's very important to look into the totality of the data. And we have these 4 trials. And for me, it's relevant to say that HEART-FID and CONFIRM are mainly for patients in the outpatient setting. And then we have AFFIRM and IRONMAN, which are either in the hospital setting or just after a recent hospitalization. So it's good to understand that the guidelines are providing us this evidence, a type IA to treat our patients with IV iron, not only in the outpatient setting, but also in the in-hospital setting. So it’s all across the pathway of our patients where IV iron seems to be very valuable.
Dr. Giuseppe Rosano:
Yes. And also what is important, I think, is that the data expand from reduced ejection fraction also to mildly reduced ejection fraction. So up until now we thought to focus mostly with iron deficiency in reduced and the data of the meta-analysis clearly showed that there is an efficacy also in the in the mid-range, which is important.
Well, this has certainly been an enlightening conversation, but before we wrap up, can you share one take-home message with our audience? Let's start with you, Ovidiu.
Dr. Ovidiu Chioncel:
So we are in a good moment now to discuss about treatment of iron deficiency. I would like to remind everyone that we have quite similar results in terms of correction of iron deficiency in terms of ferritin, of transferrin saturation. And at the end of the day, we are treating patients with heart failure and associated comorbidity, as Giuseppe presented here at the beginning. Iron deficiency treated with IV ferric carboxymaltose, totality of evidence are going in the same direction. I think that it's very encouraging for clinicians to start to identify, to assess, and to treat iron deficiency.
Dr. Antoni Bayés-Genís:
Yeah. So my take-home message would be that we need to look for iron deficiency both in the chronic setting and in the hospital, because we will see that more often than we expect. And the evidence and the guidelines recommend us IV iron in this setting. So I think we need to pay more attention to the presence of iron deficiency in spite of normal hemoglobin levels.
Dr. Giuseppe Rosano:
Thank you. And that's all the time we have today. So I want to thank our audience for listening. And I want to thank Dr. Ovidiu Chioncel and Dr. Antoni Bayés-Genís for joining me and sharing all their valuable insights. It was great speaking to you today. And thank you very much.
Dr. Ovidiu Chioncel:
Thank you.
Dr. Antoni Bayés-Genís:
Thank you very much.
Dr. Metra:
Hello, I am Dr. Marco Metra. I'm Professor at the University of Brescia, Italy. It's a pleasure for me to be here. I thank you for your kind invitation to this outstanding initiative that will help for the implementation of an effective treatment for the patients with heart failure.
Announcer:
Can you tell us about the recent updates to the ESC guidelines and how they relate to treating patients with heart failure and iron deficiency?
Dr. Metra:
We updated the guidelines based on the results of new trials published since 2021 to March 2023. And we had a new trial, IRONMAN, with ferric derisomaltose, which gave results that were consistent with the previous trials with the ferric carboxymaltose. And therefore, the results of the trials with ferric carboxymaltose were further supported by this new trial. And we had essentially 2 new recommendations regarding iron therapy for patients with iron deficiency, HFmrRF [heart failure with mildly reduced ejection fraction] and HFrEF [heart failure with reduced ejection fraction]. The first one is a recommendation to correct iron deficiency to improve symptoms and quality of life. This has become a Class I with the level of evidence A. So it's something that must be done because we have all these trials showing a consistent improvement in symptoms and quality of life. And we know that for many patients with heart failure, quality of life is more important than quantity of life. The second recommendation is to administer IV iron ferric carboxymaltose or ferric derisomaltose to reduce heart failure hospitalizations. This is a class IIa level of evidence A recommendation so means that it should be administered to reduce heart failure hospitalizations to patients with iron deficiency. And again, this comes from the priors showing an impact of treatment on heart failure hospitalizations. AFFIRM-AHF with ferric carboxymaltose was in patients recently hospitalized for heart failure. IRONMAN was in patients, also some ambulatory patients. The results were consistent. We had 4 meta-analyses showing a very consistent reduction in recurrent heart failure hospitalization, heart failure events, and cardiovascular mortality. So we have this recommendation.
Announcer:
What were the results of HEART-FID, and what can we learn from the outcomes of this trial?
Dr. Metra:
These trials were highly consistent. Now all the results are very consistent for heart failure hospitalizations. The ongoing FAIR-HF trial will give us also data with respect of mortality, but I think that now the results are very consistent from this point of view. We have had at this Congress the presentation of HEART-FID, that's a trial done in United States with iron therapy, and this is an interesting example of our statistics. And the prespecified outcome can lead to different interpretation of what are the results in the end. Meaning that also in this trial there was a reduction in heart failure hospitalizations with iron repletion therapy, except that it did not reach the P < 0.01 prespecified the significance according to the regulators. But again, the results are consistent, and above all that, the Ponikowski meta-analysis is putting together all these trials including HEART-FID, confirms the reduction of heart failure hospitalizations with iron therapy. So we have a consistency of all the trials.
Announcer:
How do the data from the current meta-analysis of the use of iron in iron-deficient patients with heart failure impact the current body of evidence, and what is the value of using IV iron to treat iron-deficient patients with heart failure?
Dr. Metra:
I think that, luckily enough, the data are reassuring, and they further confirm and make more consistent the results that were obtained in the previous trials. So they are on the same, there is no heterogeneity shown and the results are consistent. So again, we have a treatment that reduces heart failure hospitalizations in patients with iron deficiency and heart failure.
The only thing I would like to see in the future is an extension also to the patients with preserved ejection fraction because there is no reason to think that such a treatment is not effective in these patients who are actually often older, more frail, more likely to be females, so they should respond to the treatment as well.
So thank you for the invitation. Again, congratulations for the program that will help hopefully to implement an effective treatment for the patients with heart failure.
Announcer:
You have been listening to CME on ReachMD. This activity is provided by Medtelligence.
To receive your free CME credit, or to download this activity, go to ReachMD.com/Medtelligence. Thank you for listening.
 In support of improving patient care, Global Learning Collaborative (GLC) is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team.
In support of improving patient care, Global Learning Collaborative (GLC) is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC) to provide continuing education for the healthcare team.













Facebook Comments